Appendicitis Fluid In Paracolic Gutter

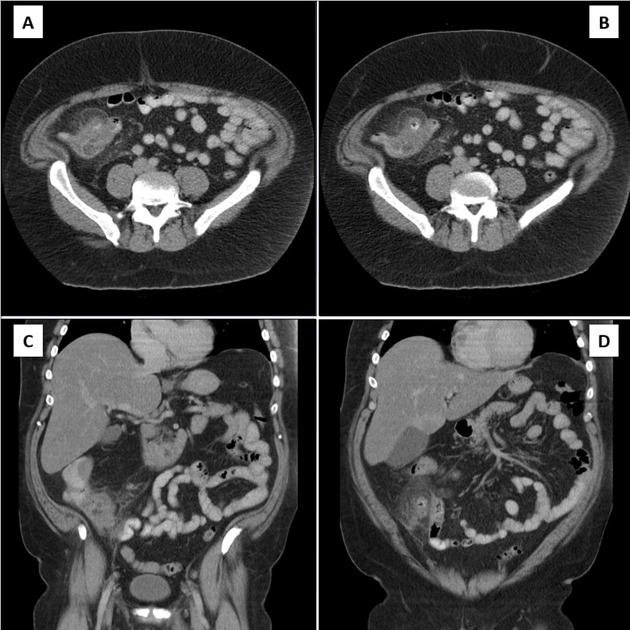
Pancreatic Injury Post Laparoscopic Subtotal Colectomy There Is Pancreatic Fluid Tracking From The Pancreatic Tail Arrows To Th Colectomy Abdomen Pancreatic

Recurrent Appendicitis After Appendectomy Cmaj
Acute Appendicitis Presenting As Urinary Retention In A Pediatric Patient

Medpix Case Appendicitis
Https Ispub Com Ijra 3 2 8205

Acute Appendicitis Radiology Case Radiopaedia Org

10 an inflamed appendix demonstrates restricted diffusion 10 the appendix may be filled with high t2 fluid or edema which decreases in signal intensity if the fluid is.
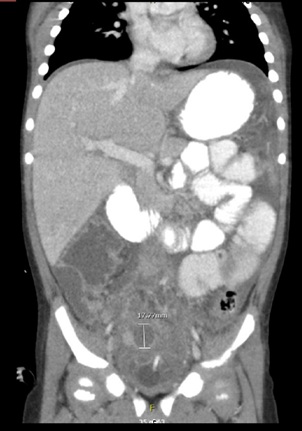
Appendicitis fluid in paracolic gutter.

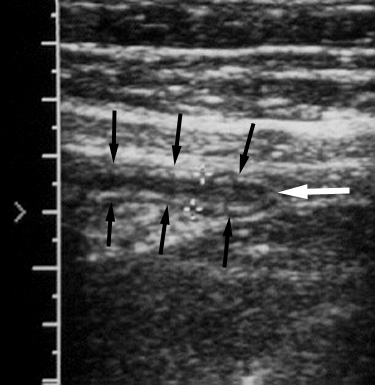
Figure 3 From Sonographically Detected Free Appendicolith As A Sign Of Retrocecal Perforated Appendicitis In A 2 Year Old Child Semantic Scholar
Stump Appendicitis Radiology Reference Article Radiopaedia Org
Associated Us Findings

Postpartum Appendicitis Presenting As Ruq Pain Letters To The Editor American Family Physician

Tuberculosis Of The Appendix Radiology Case Radiopaedia Org
Https Onlinelibrary Wiley Com Doi Pdf 10 7863 Jum 1992 11 5 209
Perforated Appendicitis Retrocecal Appendix Radiology Case Radiopaedia Org

Stump Appendicitis Radiology Reference Article Radiopaedia Org

Spleen Figure 1 Ultrassonografia Veterinaria Pinterest

Pin On Uz Skany

Role Of Multidetector Computed Tomography Mdct In Diagnosis Of Subhepatic Appendicitis Sciencedirect

Right Lower Quadrant Pain Appendicitis Nbme Surgery Shelf Exam Lower Gi Flashcards Memorang
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 102810

Appendicitis Symptoms Pathogensis Differential Diagnosis Treatment

Tuberculous Appendicitis Terminal Ileitis And Necrotic Mesenteric Lymph Nodes Radiology Case Radiopaedia Org
Valentino Syndrome Radiology Reference Article Radiopaedia Org

The Radiology Assistant Ultrasound In Acute Abdomen

Sonography In The Evaluation Of Acute Appendicitis Pacharn 2010 Journal Of Ultrasound In Medicine Wiley Online Library
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gctspc9lktrjxgnukhzt6jrmb8kwz8jsmoprhjnj4apne27o4f7i Usqp Cau

Gangrenous Appendicitis A Rare Presentation Of Pericecal Hernia Case Report And Review Of The Literature Abstract Europe Pmc

Helical Ct Of Appendicitis And Diverticulitis Sciencedirect

Pdf Iatrogenic Injury To A Vesicourachal Diverticulum During Laparoscopic Appendectomy Successfully Managed Conservatively

Pdf Stump Appendicitis A Comprehensive Review Of Literature

Longitudinal Appendix Ultrasound Sonography
Source : pinterest.com
